|
Bangabandhu Sheikh Mujib Medical University Journal Volume 17, Issue 1, March 2024
CASE REPORT Intrauterine fetal death
product as a foreign body in the urinary bladder: A case report
Md. Abu Nahid
Department of Urology, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh.
DOI: https://doi.org/10.3329/bsmmuj.v17i1.63280 Received: 13 Dec 2022; Revised version received: 23 Jan 2024; Accepted: 29 Jan 2024 Published online: 15 Feb 2024 Responsible Editor:
M Mostafa Zaman |
INTRODUCTION
Foetal death is defined as death prior to the complete expulsion or extraction from its mother of a product of human conception, irrespective of the duration of pregnancy and not an induced termination of pregnancy.1 Intrauterine foetal death (IUFD) is managed by delivering the foetus though the method and timing of delivery depends on the gestational age.2 Currently, there is a paucity of literature regarding the natural history of the IUFD of foetuses in humans. D Aunoy and King have listed four changes a foetus may undergo if it is not expelled out or removed: (a) Skeletonization, where the soft parts undergo disintegration; (b) Adipocerous, where the soft parts are replaced by fatty acids soaps and salts; (c) Suppuration, where an abscess is formed, usually due to E. coli infection; (d) True lithopedion formation (stone baby) if the foetus remains in a sterile environment.3 To date, there is no literature reporting the migration of the foetal part following an IUFD from the uterus to the abdomen, urinary bladder (urinary bladder), or another part of the abdominal cavity naturally if the foetus was not removed.
The foetus itself is antigenically foreign to the mother. After an IUFD, it functions as a foreign body to be expelled. All foreign bodies tend to be absorbed, abolished, and expelled.4
Foreign bodies in the urinary bladder are relatively rare.5 There is one case report whereby foetal bone was found within the urinary bladder as foreign body with a history of IUFD treated by dilatation and curettage seven years back.6
Here, we are presenting a rare case where a woman has presented to us with foetal bone as foreign body within abdominal cavity and urinary bladder following migration from uterus with a history of IUD at 27th weeks of gestation for which she did not received any treatment about 17 years back.
LEARNING POINTS
1. Migration of intrauterine foetal death products from uterus to the urinary bladder may I happen, although it is very rare.
2. Diagnosis can be done with a careful history taking and relevant imaging techniques.
3. Hysterectomy and cystectomy may be necessary protecting the organs having adherence with the growth.
CASE DESCRIPTION
A 54 years old, non-diabetic, normotensive female, got admitted to the Department of Urology, BSMMU, with the complaints of passage of hard bony fragment like materials with urine through external urethral meatus for last 4 months. She also complained of hesitancy, intermittency, and occasional dysuria for the same duration.
She had a history of IUD at 27 gestational weeks about 17 years back. She was admitted to a local hospital and advised for induction of labor for foetal expulsion but could not continue treatment for poor socio-economic conditions.
Three months later, foul-smelling fleshy materials were expelled out per vagina, which lasted for 4-5 days and subsequently resolved spontaneously. It was her 8th gravida. She had a regular menstrual cycle till the age of 52 years.
Here, we are presenting a rare case where a woman has presented to On examination, She had a hard round abdominal lump of about 4x3 cm in diameter at the midline of the umbilical region, fixed with the abdominal wall, moved side to side but not above downward.
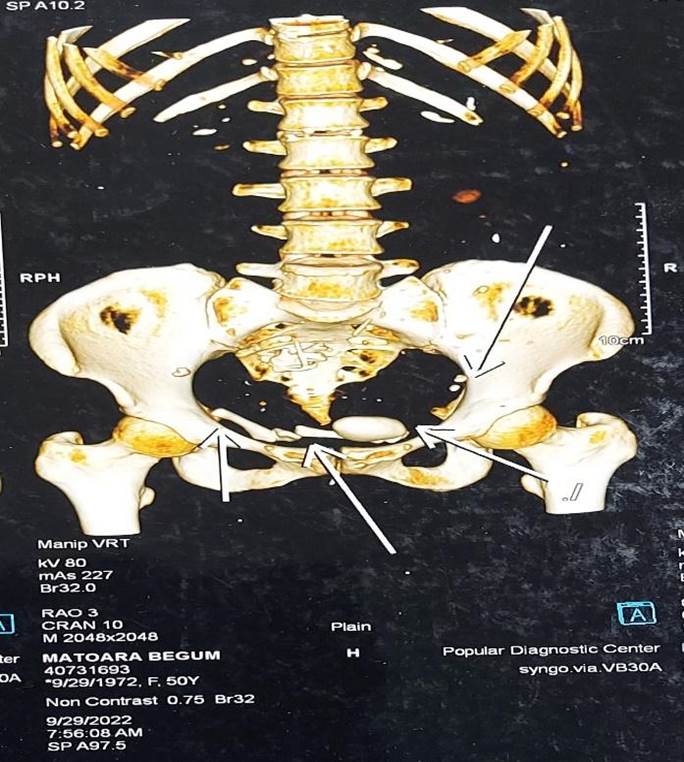
A plain X-ray of the kidney and urinary bladder revealed one large and two small, rounded radio-opaque shadows in the pelvic cavity (Figure 1). An Ultrasonogram of the whole abdomen revealed a thick, irregularly walled urinary bladder, low-level echoes, and a few bright echogenic structures casting posterior acoustic shadow within the Urinary Bladder and hyperechoic irregular endometrium. A contrast CT scan of KUB revealed foetal skeletal parts within the urinary bladder cavity and its wall, intestine, urethra, uterine cavity, pelvic cavity, and involved abdominal wall (Figure 2).
CASE MANAGEMENT
Urethro-cystoscopy revealed multiple bony parts floating within the urinary bladder, a large stone, and an area of unhealthy granulation tissue involving the dome and posterior wall of the urinary bladder. Guidewire could not be negotiated through the unhealthy area. The vaginoscopy revealed no abnormality.
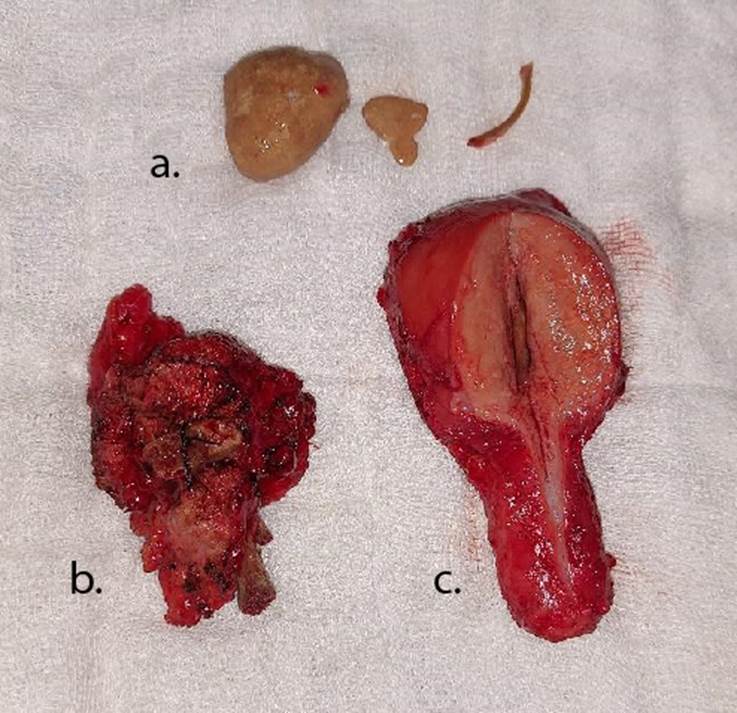
Laparotomy was done using a lower midline incision over the mass. While entering the abdomen, a hard growth of 4x3 cm was found fixed with the rectus abdominis muscle containing foetal bony parts. The growth was also adhered to the urinary bladder wall, uterus, and ileum. The growth was separated from the ileum. Total abdominal hysterectomy and partial cystectomy were done. A vesical stone and multiple foetal bony parts were extracted from the urinary bladder, followed by bilateral Double-J stenting along with repair of the bladder wall (Figure 3).
Her postoperative period was uneventful. After the removal of the catheter on the 14th postoperative day, she was discharged with a follow-up scheduled at 3 months.
A histopathological examination of the uterus done by the Department of Pathology, Bangabandhu Sheikh Mujib Medical University revealed chronic cervicitis with squamous metaplasia and ulcer. Specimen of bladder tissue and foreign body granuloma revealed foci of ulcer lined by granulation tissue and infiltration of chronic inflammatory cells but there were malignant cells.
DISCUSSION
This may be the first instance in Bangladesh of natural migration of foetal remnants of IUD outside of the uterus. As a foreign body, an IUD product erodes from the uterus towards the abdominal cavity involving the ileum and abdominal wall. Any foreign body inside the body wall can potentially migrate in any direction, particularly to the urinary bladder, if it is near it.7
In this case, the dead foetus within the uterus underwent disintegration followed by suppuration, leading to perforation of the uterus. The bony parts migrated through the uterine perforation into the pelvic cavity. Some of the migrated foetal bones acted as a nidus for granuloma formation, giving rise to the hard lump found in the anterior abdominal wall and severe adhesion between the ileum, abdominal wall, and urinary bladder. Some of the foetal bones remain adhered to the anterior uterine wall and urinary bladder. Eventually, the uterine perforation was healed, and the bony fragments eroded the urinary bladder and settled in the bladder cavity. Hence, there were no symptoms of vesico-uterine fistula. Due to the foreign body in the bladder wall, the patient had both irritative and obstructive symptoms.
Various urinary bladder foreign bodies have been reported in the literature but migration of remnant of IUD to urinary bladder is not yet reported. Therefore, patients with LUTS and abnormal urinary content should be evaluated with previous clinical history and relevant examinations, and managed accordingly. A foreign body in the urinary bladder remains a great challenge to the urologist. Its removal without causing an injury to the urinary bladder or the urethra gives a good outcome.
Acknowledgments
We are thankful to the patient for her co-operation during the treatment & follow-up period.are thankful to the patient for her co-operation during the treatment & follow-up period.
Author contributions
Conception and design: MAN, MH. Acquisition, analysis, and interpretation of data: MAN, MH, MSI. Manuscript drafting and revising it critically: MAN, MH, NI, MURAM, MSI. Approval of the final version of the manuscript: MAN, MH, NI, MURAM, MSI. Guarantor of accuracy and integrity of the work: MAN, NI.
Funding
This study did not receive any external funding.
Conflicts of interest
The authors have no conflict of interest to declare.
Ethical approval
The authors took consent from the patient to participate in this study.
Data sharing
The data that support the findings of this study are available on request from the corresponding author.
References
1. Management of Stillbirth: Obstetric Care Consensus. American College of Obstetricians and Gynecologists. No, 10. 2020 Mar;135(3):e110-e132. doi: https://doi.org/10.1097/AOG.0000000000003719. Erratum in: Obstet Gynecol. 2023 May 1;141(5):1030.
2. Dave A, Patidar R, Goyal S, Dave A. Intrauterine foetal demise-a tragic event: A study of its epidemiology, causes and methods of induction. International Journal of Reproduction, Contraception, Obstetrics and Gynecology, 2016;1316-1321. DOI: https://doi.org/10.18203/2320-1770.ijrcog20161008.
3. Gedam BS, Shah Y, Deshmukh S, Bansod PY. Skeletal remains of mummified foetus for 36 years in mother's abdomen. International Journal of Surgery Case Reports, 2015;7:109-111. DOI: https://doi.org/10.1016/j.ijscr.2014.10.074.
4. Odoemene CA, Onuh CA. Foreign bodies in the urinary bladder-case series. J West Afr Coll Surg. 2017 Jul-Sep;7(3):124-136. PMID: 30525007.
5. van Ophoven A, deKernion JB. Clinical management of foreign bodies of the genitourinary tract. J Urol. 2000 Aug;164(2):274-287. DOI: https://doi.org/10.1097/00005392-200008000-00003.
6. Malik MA, Rehan AG, Ahmad I, Ahmad T. Foetal Bone as a foreign body in the urinary bladder: A case report. Journal of Medical Case Reports. 2009;3(1):8994. DOI: https://doi.org/10.4076/1752-1947-3-8994.
7. Mylarappa P, Srikantaiah HC. Calcified intravesical gossypiboma following abdominal hysterectomy: a case report. J Clin Diagn Res. 2011;5:645-647. Available at: https://www.jcdr.net/articles/pdf/1366/2259~final.pdf
|
|
|
FIGURE 1 Plain X-ray of kidney, ureter and bladder region |

|
|
|
|
A |
B |
|
Figure 2 a. Reconstructed film of CT, and b. Coronal section of kidney ureter and bladder region |
|

|
|
|
FIGURE 3 a. Vesical calculus and foetal bony parts retrieved from bladder; b. Partial cystectomy specimen and foreign body granuloma; c. Specimen of total abdominal hysterectomy |
(c) 2024 The Authors. Published by BSMMU Journal