Bangabandhu Sheikh Mujib Medical University Journal
Volume 16, Issue 4, December 2023
CASE REPORT
Sealing coronary perforation
by hand-made covered stent: A case report![]()
Md. Fakhrul Islam Khaled1*![]() , Muhammad
Salim Mahmod
, Muhammad
Salim Mahmod![]() 2, Mohammad
Arifur Rahman3
2, Mohammad
Arifur Rahman3![]() , Mohammad
Moynul Haque1, Sharmin Ahmed1
, Mohammad
Moynul Haque1, Sharmin Ahmed1![]()
1Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh; Email: drfikhaled@bsmmu.edu.bd, sharmin.disha@gmail.com
2Dr. Sirajul Islam Medical College Hospital. Dhaka, Bangladesh; Email: maheccc@gmail.com
3Sarkari Karmachari Hospital, Dhaka, Bangladesh; Email: drarif79@yahoo.com
*Correspondence: Dr Md. Fakhrul Islam Khaled; Department of Cardiology; Bangabandhu Sheikh Mujib Medical University; Dhaka, Bangladesh
DOI: http://doi.org/10.3329/bsmmuj.v16i4.67399
Received: 3 July 2023; Revised version received: 18 Oct 2023; Accepted: 19 Oct 2023; Published online: 9 Nov 2023
![]()
ABSTRACT
Coronary artery perforation, a rare but deadly complication of percutaneous coronary intervention (PCI), can be managed by several modalities, including balloon inflation, heparin-reversing agent, thrombin injection, microcoils, fat embolization, covered-stent implantation, or surgery. We share our experience in emergency innovative management of coronary perforation during routine PCI. We faced an Ellis class III perforation of the right coronary artery during PCI. The balloon inflation technique failed to occlude the perforation, and no other facility was available to solve the problem immediately. The patient developed mild pericardial effusion but was hemodynamically stable. We made a covered stent by wrapping it with polyurethane (Tegaderm(R) skin dressing material) and deployed it. The perforation was sealed. The patient was discharged in stable condition and doing well at a 12-month follow-up examination. Hand-made covered stent may be a good bailout option to seal coronary perforation where premounted covered stents are not readily available.
Keywords: percutaneous coronary intervention, coronary artery perforation, covered stent
Highlights
1. Coronary artery perforation during a percutaneous coronary intervention is a potentially deadly complication that warrants knowledge and skills to manageit.
2. A hand-made Tegaderm(R) wrapped stent may be a good bailout option to manage coronary perforation where premounted covered stents are not readily available.
INTRODUCTION
Coronary artery perforation (CAP) is a deadly complication of percutaneous coronary intervention (PCI), though the chances are very low (0.1% to 0.5%)1. Various modalities exist to treat CAP, such as balloon inflation, thrombin injection, microcoils, covered-stent implantation, and surgery. Each method has some benefits and drawbacks. Balloon inflation seals the perforation and maintains distal vessel flow. This method occasionally fails to close the perforation completely. Covered stents are significantly more effective in sealing CAP than balloon inflation, but it is not widely available. Moreover, a covered stent may increase the risk of stent thrombosis or in-stent restenosis. Tegaderm(R) is made of a thin polyurethane membrane layer used for aseptic skin dressing. Tegaderm-wrapped stents can be considered a new innovative life-saving emergency tool to treat deadly coronary perforation and can be hand-made in the catheterization laboratory (cath-lab)2.
CASE DESCRIPTION
A 50-year-old hypertensive, diabetic, and dyslipidaemic man was admitted with complaints of moderately severe effort angina for several months with stable hemodynamics and without any remarkable clinical abnormalities. The complete blood count and serum creatinine level were within normal limits. A 12-lead electrocardiogram and echocardiography revealed normal findings with good bi-ventricular systolic function. A coronary angiogram done through the right radial route in Dr. Sirajul Islam Medical College Hospital, Dhaka, revealed 80 - 90% stenosis of proximal to mid-left anterior descending artery (LAD) and 90 - 95% long stenosis to mid-right coronary artery (RCA) (FIGURE 1a).
CASE MANAGEMENT
Angioplasty to the LAD and RCA with a drug-eluting stent was planned. LAD was wired with Fielder FC(R), predilated with a 2x15 mm compliant balloon, and a 3x24 mm drug-eluting stent was deployed. Post-procedure thrombolysis-in-myocardial-infarction grade-3 (TIMI-3) flow was achieved in LAD. RCA was wired with floppy wire and sequentially predilated by 1.5x12, 2x12 mm compliant balloon. A drug-eluting stent of 2.5x30 mm size was tried to deploy but failed. Then, a 2.5x12 mm non-compliant balloon was used for appropriate pre-dilatation. Then, an Ellis type-III perforation was observed in mid-RCA (FIGURE 1b). A balloon was kept inflated at the perforation site, but the leakage was not sealed. The patient’s hemodynamics remained stable, though minimal pericardial effusion was observed. Our next treatment options were either emergency coronary artery bypass surgery or a covered stent deployment. Unfortunately, neither the cardiac surgery team nor the covered stent was available instantly. We made a covered stent by Tegaderm(R) (polyurethane) available in the cath lab for aseptic dressing.
Meanwhile, an inflated balloon was kept at the perforation site to prevent progressive leakage. We cut polyurethane skin dressing material at size 2 mm less length of the stent, wrapped two-fold over the stent (FIGURE 2a), and changed the guide catheter to 7 Fr sized XB(R) to deploy the stent. The hand-made covered stent was deployed at 14 ATMs. No further extravasation (FIGURE 2b) was observed. Finally, the patient was discharged per the hospital’s standard practice. The patient was found stable at a one-year follow-up. He was reportedly doing his professional activities without any major limitations.
DISCUSSION
The CAP during PCI may result in grave clinical outcomes, such as pericardial tamponade, myocardial infarction, need for emergency coronary artery bypass surgery, or death.3, 4 Several factors predispose to CAP, such as excess vessel tortuosity, narrow vessel diameter, presence of calcification, chronic total occlusion, use of an oversized balloon, and high-pressure balloon dilatation.5 Classical nonsurgical management for type III perforation often fails, requiring coronary stent or surgical intervention.4, 5 The use of a covered stent can defer emergency surgery in such a life-threatening situation. Covered stent has a long history in interventional cardiology for the management of coronary perforations and occluding coronary aneurysms.6 Covered stents from various materials are commercially available, such as polytetrafluoroethylene, polyurethane, and pericardium.7 High occurrence of in-stent restenosis (25%) and stent thrombosis (3% to 16%) long-term after polytetrafluoroethylene-made coronary stent signifies its poor outcome.8 Nowadays, polyurethane is used progressively in cardiac prosthetics like ventricular assist devices and prosthetic valves.9 Recently, coronary perforations have been treated by pericardial-covered stents.10 A self-made polyurethane coronary stent is considered an alternative to the premounted coronary stent to treat coronary perforation. Polyurethane membrane, a covering material, is widely available in cath labs and can be wrapped over appropriately sized stents within a short period and deployed with a higher-sized guide catheter (7 Fr). The procedure can be continued after proper sealing of the perforation sites using covered stent, and there is no need to reverse postprocedural standard antiplatelet and anticoagulant strategies.2 The potential risks and limitations are maintenance of sterility and drug-coating of the stent. Therefore, this technique can be considered as a bail-out procedure and not for routine practice.
The present case reminds us that coronary perforation can occur during any calcified lesion intervention. CAP is a potentially deadly complication, and familiarity with the steps to manage this complication is essential. Appropriate preparation to combat this type of emergency should be kept in the cath lab. Hand-made covered stent may be a good bailout option to manage coronary perforation where premounted covered stents are not readily available. However, further research on the long-term outcome of this procedure is warranted.
Acknowledgments
We thank Professor Sajal Krishna Banerjee, University Grants Commission, Bangladesh, Professor SM Mostafa Zaman, Department of Cardiology, BSMMU, and the concerned team members of Dr. Sirajul Islam Medical College Hospital, Dhaka.
Author Contributions
Conceived and designed the experiments: MFIK, MMH. Performed the experiments: MFIK, MMH, MSM, MAR. Manuscript writing and revising: MFIK, SA. Approval of the final version: MFIK, MAR, MSM. Guarantor accuracy and integrity of the work: MFIK, MMH.
Funding
No funding support was received for this work.
Conflicts of Interest
The authors declare no conflict of interest.
Ethical Approval
Because the current manuscript is a case based on an emergency life-saving procedure, we did not ask for ethical approval but obtained written consent from the patient for this publication.
ORCID iDs
Md. Fakhrul Islam Khaled https://orcid.org/0000-0002-1003-6598
Muhammad Salim Mahmod https://orcid.org/0009-0007-1194-6925
Mohammad Arifur Rahman https://orcid.org/0000-0003-0840-4213
Sharmin Ahmed https://orcid.org/0000-0002-3111-0849
References
1. Rakowski T, Węgiel M, Siudak Z, Plens K, Dziewierz A, Birkemeyer R, Kleczyński P, Tokarek T, Rzeszutko Ł, Dudek D. Prevalence and Predictors of Coronary Artery Perforation During Percutaneous Coronary Interventions (from the ORPKI National Registry in Poland). Am J Cardiol. 2019 Oct 15;124(8):1186-1189. DOI: https://doi.org/10.1016/j.amjcard.2019.07.021.
2. Song X, Qin Q, Chang S, Xu R, Fu M, Lu H, Ge L, Qian J, Ma J, Ge J. Clinical Outcomes of Self-Made Polyurethane-Covered Stent Implantation for the Treatment of Coronary Artery Perforations. J Interv Cardiol. 2021 May 17;2021:6661763. DOI: https://doi.org/10.1155/2021/6661763.
3. Ellis SG, Ajluni S, Arnold AZ, Popma JJ, Bittl JA, Eigler NL, Cowley MJ, Raymond RE, Safian RD, Whitlow PL. Increased coronary perforation in the new device era. Incidence, classification, management, and outcome. Circulation. 1994 Dec;90(6):2725-2730. DOI: https://doi.org/10.1161/01.cir.90.6.2725.
4. Briguori C, Nishida T, Anzuini A, Di Mario C, Grube E, Colombo A. Emergency polytetrafluoroethylene-covered stent implantation to treat coronary ruptures. Circulation. 2000 Dec 19;102(25):3028-3031. DOI: https://doi.org/10.1161/01.cir.102.25.3028.
5. Al-Mukhaini M, Panduranga P, Sulaiman K, Riyami AA, Deeb M, Riyami MB. Coronary perforation and covered stents: an update and review. Heart Views. 2011 Apr;12(2):63-70. DOI: https://doi.org/10.4103/1995-705X.86017.
6. Jamshidi P, Mahmoody K, Erne P. Covered stents: a review. Int J Cardiol. 2008 Nov 28;130(3):310-318. DOI: https://doi.org/10.1016/j.ijcard.2008.04.083.
7. Javaid A, Buch AN, Satler LF, Kent KM, Suddath WO, Lindsay J Jr, Pichard AD, Waksman R. Management and outcomes of coronary artery perforation during percutaneous coronary intervention. Am J Cardiol. 2006 Oct 1;98(7):911-914. DOI: https://doi.org/10.1016/j.amjcard.2006.04.032.
8. Lee WC, Hsueh SK, Fang CY, Wu CJ, Hang CL, Fang HY. Clinical Outcomes Following Covered Stent for the Treatment of Coronary Artery Perforation. J Interv Cardiol. 2016 Dec;29(6):569-575. DOI: https://doi.org/10.1111/joic.12347.
9. Maluf MA. New polyurethane prostheses for substitution of cardiac valve disease and remodeling of the right ventricle in congenital heart malformations. J Cardiothorac Surg. 2013 Sep 11;8(Suppl 1):O141. DOI: https://doi.org/10.1186/1749-8090-8-S1-O141.
10. Jokhi PP, McKenzie DB, O'Kane P. Use of a novel pericardial covered stent to seal an iatrogenic coronary perforation. J Invasive Cardiol. 2009 Oct;21(10):E187-90. PMID: 19805849.
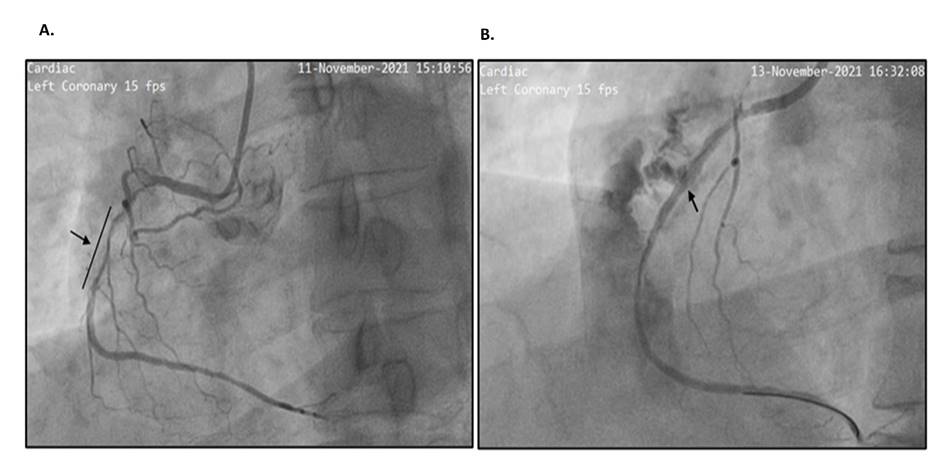
FIGURE 1 Lesion in the right coronary artery: (a) 90-95% long stenosis in proximal to mid-segment. (b) Perforation in right coronary artery (pointed).
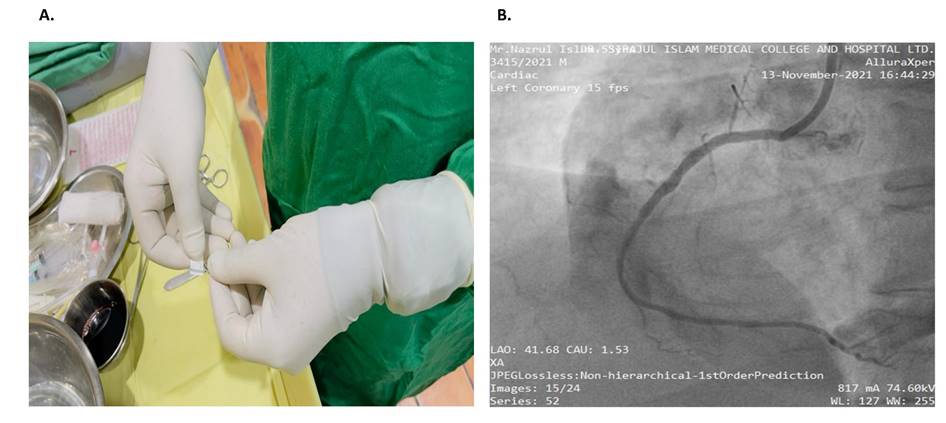
FIGURE 2 Case management (a) Wrapping of Tegaderm(R) cover stent; (b) After deployment of hand-made covered stent no leaking is visible
(c) 2023 The Authors. Published by BSMMU Journal